I'm always fascinated when health care discussions start up on HN; watching Americans argue amongst themselves about single-payer or nationalized health care systems as if those systems are dangerous thought experiments are mesmerizing.
No matter how many people say "but a well regulated mandatory multi-payer type of system is working in Germany" or "nationalized medicine is working in Canada" it's all just ignored and the argument continues anew.
>No matter how many people say "but a well regulated mandatory multi-payer type of system is working in Germany" or "nationalized medicine is working in Canada" it's all just ignored and the argument continues anew.
I don't think their problem (at least of one side of the debate) is whether it will work or not.
Their issue is a moral one, whether they should ever pay into a health care pool for the benefit of other people.
Those that think they can manage on their own don't see why that should happen. And as a protestant inspired culture that took it even further than the original protestants, they find this appalling.
They'd rather see people die in the streets and step over them on the way to brunch, than have themselves, hardworking "good" persons that they are, contribute for the health of the poor and the "losers". Even more so if it's mandatory. Charity from their magnanimous heart, they can consider.
I'd posit that the morale and cultural issue is exacerbated in mid- to lower-income brackets by the ever tightening costs of surviving in modern society.
The fact people in general can barely maintain their own needs makes it even more of a struggle to sell helping everyone else in general (healthcare, fire departments, schools...). They, themselves, would like financial assistance but can't get it so have quite a bit of resentment (and who can blame them for that).
If most folks had more resources (e.g. money), I think you'd find the culture would shift a reasonable amount towards supporting things like universal healthcare, etc. In a culture driven by constant economic competition for survival, it makes sense that people don't want to help their potential economic enemies. If there's fewer people, there's less competition, less kids to grow up and displace them, etc.
There are still people who literally do not have any concern for the wellbeing of others and no amount of resources would change their perspectives but I argue those are relatively few in the general population.
This mindset does not make sense to me. People already pay for local schools (K-12), even if they have no children. They already pay for a local library, even if they never use it. They pay for a local fire department, even if their house never burns down. They pay for a local police station, even if they are never the victim of a crime.
People pay for services that benefit others all the time - why should health be any different?
> People already pay for local schools (K-12), even if they have no children.
Very rarely. Good schools attract paying parents with large families, leading to a self-reinforcing effect and affecting property values so much that it's one of the search facets on property sites like Zillow. So really they pay for their children, usually.
> They already pay for a local library, even if they never use it.
This is a relic of when people did use libraries more. A lot of library systems are dying out with the excuse of "but we prefer Kindles".
> They pay for a local fire department, even if their house never burns down. They pay for a local police station, even if they are never the victim of a crime.
They do this more out of fear of avoiding viscerally life-threatening consequences. Somehow healthcare has assumed the status of not such a thing in the States.
-----------
For what it's worth, I am strongly opposed to these viewpoints, but just stating that there is not as much self-contradiction there as you think.
What do you mean people “very rarely” pay for local schools? I pay over 50% of my local property taxes into the school district here. It’s roughly that much all over the city and all over any big city in my state; you can’t escape it. And it was about $2800 out of my pocket last year.
And if you’re not paying this directly, it’s probably because you rent (and you’re getting passed on the cost) or it’s hidden in income taxes.
> What do you mean people “very rarely” pay for local schools?
I guess a nuanced version of what I mean is – they very rarely pay a lot for schools if they don't have children. Put another way, they do pay through the nose for schools if they do have children, which it sounds like you are doing.
Of course there are exceptions to this. Maybe you live in a district with great schools and have no children, in which case you are paying for a great school with no direct way you can take advantage of the benefits. My point was that this situation is relatively rare; perhaps it wasn't expressed too well.
>People pay for services that benefit others all the time - why should health be any different?
If some people could have their way, they'd remove paying for those -- or for bridges, roads, federal infrastructure etc away from their area, too. Let the locals short it out.
But a difference with those things you've mentioned is that they were born with them existing. So they're some kind of default (though a minority still debates them). Whereas nationalized healthcare would be a new development for them....
Believe me, they don't want to pay for these. We, in Fl, have people move into the state and fight their property tax because "our kids are not in school anymore".
What I don't understand is why people would need to pay more (and that always seems to be the crux of why we can / can't do something). It's about allocation of existing funds to me. We spend more on our military than most other other developed nations combined. There are other billions of dollars misappropriated. Bolstering the coffers with taxes is simple, but doesn't seem entirely necessary since there is already a ton of money floating around.
You would need to pay more in the short term when transitioning, but not in the long term. You spend far and away more on health care per capita than any other country in the world.
Exactly the point. K-12 public education is a huge waste of money and that nets poor results. Nobody wants to pay for private healthcare on top of private education that is near-mandatory in some parts of the country
> Exactly the point. K-12 public education is a huge waste of money and that nets poor results. Nobody wants to pay for private healthcare on top of private education that is near-mandatory in some parts of the country
Having children is a choice at a different level than the need for healthcare. If I had to pick between public education and public healthcare, I'd pick public healthcare every time.
I haven't verified it but a quick Google search shows "American taxpayers spent close to $649 billion on its K-12 schools in 2015".
I don't know how much the US spends on healthcare. iirc it is about 18% of GDP or roughly a fifth. If our GDP is USD 20T, then we already spend almost $4T on healthcare. We don't know if adopting a system similar to Germany's will allow us to get it down to what Germany has (11% of GDP) but we have to try.
They are though. The US are among the top countries in the world in $/capita from public (tax) funding towards healthcare. And then they add a stack of about the same size of private funding.
Americans pay about twice as much as all other western nations for the opportunity to turn people away. It's not about contributing for the health of losers, it's about being ok with paying double so that losers don't get anything.
This belief that it's about not wanting to pay needs to end. They are paying just as much as everyone else from taxes, and then paying another just as big amount out of their own pockets.
Yeah, I definitely get that from the subtext or, sometimes, the text. The weird thing is that it's cutting off their noses to spite their faces ... they spend MORE on insurance then they would in taxes.
But in a lot of cases, it's like they will not (or can not) learn from what is going on in other countries. Maybe it's also US exceptionalism at play?
I think what it comes down to for many people is that their employer covers their health insurance premiums, and they fear that they would actually have to pay market value for health insurance if it were removed from the employer benefit umbrella.
For a country that supposedly values small business, there are few things I could think of that would support small business more than public healthcare. Currently, large employers can get a group plan with very reasonable rates. Small employers are pretty much out of luck.
It stands to reason to me that the bigger the pool, the more predictable and lower the costs. It's ridiculous to me that arbitrary groups of people can't go in on a health plan together. If a company with 50k employees can do it, why can't a city / state / random assortment of people?
That’s basically what the health exchanges are. Small businesses do not have to provide health insurance; and in most cases the exchanges provide more choice and lower cost than small businesses would have access to.
But it does increase the gap in wages between the big corporates and small businesses. It’s very hard for small businesses to hire good talent when they can work in the corporate world for a higher salary plus benefits.
As someone who works for a small company (~10-15 people), it's possible we're missing out on something obvious, but two years ago we (my employer) looked pretty extensively into our different options and settled on our current plan as the best option.
I have a 1500/3000 family plan with a sticker price of $32,000 / year. I pay a third of that and my employer picks up the rest. I guess it's possible that this is about the going rate and most employers just pick up more of the cost than mine.
Either way, that seems like an unsustainable amount of money to be paying each year.
Yeah, a family plan at my employer (a big corporate) with the same limits is about $5000/yr to the employee. And that’s on top of the fact my salary is already 25-50% higher than it would be at a small business. The deck is seriously stacked against smaller employers right now.
I think you can see a bit of the same thing with ID cards and unique identifiers. Most European countries have a state-issued ID card and an unique identifier for every citizen. The US has a million IDs from different institutions, states, corporations and they keep causing messes, still, having 1 ID card and a unique identifier is seen as bad for reasons that baffle me.
> Their issue is a moral one, whether they should ever pay into a health care pool for the benefit of other people.
I mean, realistically, that's what all insurance is anyway. The trouble with the US system (vs other mandatory/psuedo-mandatory insurance systems) is more around the way it's regulated.
True. We are required to pay taxes to support insurance schemes we can never use ourselves. So, in a sense, it's worse than what I stated. Payment is compulsory, but coverage is optional (and extra cost) for the majority of working Americans.
That makes me think of Braess paradox and see parallels.
(https://en.m.wikipedia.org/wiki/Braess's_paradox)
As most people seem to try to take the most optimal self-interested decision it does not always make the outcome the most optimal for them or everyone. As actions we take as not, affect more than ourselves and can't be totally disconnected from this world.
And as a individual to be able to take the most optimal decision in complex systems is pretty difficult.
What would we be without our choice and an AI or a higher power would take the decisions for us?
This mindset does not make sense to me. People already pay for local schools (K-12), even if they have no children. They already pay for a local library, even if they never use it. People pay for services that benefit others all the time - why should health be any different?
My father in law said something along the lines of "I don't know why they make us pay taxes for the public school system." So that mindset is definitely out there. (My wife and her brother got sent to a private Christian school)
I think his main issue with it is that he thinks they are wasteful with their budgets. I've never really figured it out.
That argument was discussed and resolved when the Articles of Confederation were disbanded some 200+ years ago. If anything military spending would be a good reason not too socialize anything as it has clearly gotten out of control.
That's not the same thing. Other "hard working" people are paying into private ins along with you. The poor don't because their hours are capped at 30 so they'll never get health insurance. Therefore they're not contributing, therefore they don't deserve it.
Note: This is not my position on the matter. Just trying to explain the difference.
Edit: Regarding Medicaid and Medicare - believe me, people would love to see Medicaid go also. I think they're OK-ish with Medicare because they know they'll get old at some point.
That would be great, except a large percentage of the country doesn’t make enough money to afford insurance. So they go to the ER (the most expensive form of care) and end up neck-deep in medical debt from routine health issues.
Even when you can afford it, an increasing number of doctors are refusing to accept insurance. These doctors tend to be more highly regarded and provide a higher standard of care because they’re not shackled to a computer doing insurance paperwork half the day.
So even with the system we have, insurance isn’t really worth it unless you have chronic health issues. This becomes a feedback loop of increasing prices and decreasing benefits for all but the most expensive patients.
The moral hazard isn’t in paying for it, it’s in how the profit motive multiplied across dozens of middlemen is corrosive to the quality of the system. We’re paying for it regardless, but we pay a lot more under the current system because we have to support perpetual growth of every company in the value chain.
> Those that think they can manage on their own don't see why that should happen. And as a protestant inspired culture that took it even further than the original protestants, they find this appalling.
> They'd rather see people die in the streets and step over them on the way to brunch, than have themselves, hardworking "good" persons that they are, contribute for the health of the poor and the "losers". Even more so if it's mandatory. Charity from their magnanimous heart, they can consider.
1 - A significant portion of our economy is healthcare middlemen. With single payer or nationalized care, all of our Blue Crosses and Cignas (and the jobs associated) would evaporate overnight.
I'm not arguing that we need trillions of dollars of our GDP locked up in middlemen, but it's very hard for a man to understand something when his salary depends on his not understanding it.
2 - We hear about long wait times in other countries. And the stories are mostly true. There's nothing wrong with waiting, but we've been conditioned to expect near-immediate resolutions.
People in the United States with high-quality private insurance* can usually be seen by a specialist within a few weeks regardless of how severe or immediate their problem is. The truth is that unless that person has some kind of advanced or rapidly progressing disease, they could wait for months without any problems. But that would be a major change to the way we think. It would mean allocating care based on need, not based on ability to pay.
*High-quality private insurance is usually one of the perks of working for a great company. I would argue that only a small minority of Americans have truly high-quality coverage. But all of the people who don't have high-quality coverage envy the others and vote with them, a la "temporarily embarrassed millionaire."
You are absolutely right about the middlemen/women. But don't forget to mention the doctors, nurses and PAs as well (more on doctors). They have skin in the game and most of the US doctors that I've talked to aren't that keen on single-payer system. The only excuse they have is that it'll flood the system with a lot more patients (I'm sure it can be solved the same way it is solved in Canada et al.) and that the quality of care will be reduced (can't see that rationale).
About the long wait time - I waited from 11pm until 8:30am (discharge) in the morning in ER of Strong Memorial hospital one day for falling and bleeding from my nose (I thought I broke my nose, but luckily, I didn't). I should have answered my pain level was 10 instead of being truthful about it and responding 3. This is not to mention that I got charged $250 from deductibles despite having the insurance.
My sister, who lives in Rochester, NY, is waiting until May 2020 to get an appointment for yearly physical checkup. There's a significant shortage of doctors in rural areas (Rochester isn't even that rural to be honest). And yet, AMA is happily restricting the supply of new doctors by putting up multiple hurdles including exam fees (not to mention the amount of money they charge for each USMLE exam is ridiculous) and requirement to go through 8 years of education when that could have been easily reduced to just 4 for any IM (internal medicine) physician.
> About the long wait time - I waited from 11pm until 8:30am (discharge) in the morning in ER of Strong Memorial hospital one day for falling and bleeding from my nose (I thought I broke my nose, but luckily, I didn't).
This is how the system is supposed to work. Even if you had broken your nose, unless it's some gaping open fracture or the bleeding can't be controlled, it's probably not a higher priority than most of the cases they see.
> My sister, who lives in Rochester, NY, is waiting until May 2020 to get an appointment for yearly physical checkup. There's a significant shortage of doctors in rural areas (Rochester isn't even that rural to be honest). And yet, AMA is happily restricting the supply of new doctors by putting up multiple hurdles including exam fees (not to mention the amount of money they charge for each USMLE exam is ridiculous) and requirement to go through 8 years of education when that could have been easily reduced to just 4 for any IM (internal medicine) physician.
This is a complicated problem. Our current system incents people to become specialists. Why would I want to go to school for 8 years (taking on $200-300k in student loans if I'm lucky) and then do 1-3 years of 100-hour weeks making $50k to come out making less than a twentysomething software engineer?
This. He didn’t even break his nose, so it was ... a boo-boo? Yeah, you’re gonna wait in line for that. Source: family member who works in ER, trainee in triage.
The AMA is hardly restricting the supply of new doctors. Exam fees are a tiny fraction of medical school tuition.
The real supply bottleneck is in federal funding for additional residency slots. Every year students graduate from medical school but are unable to practice because they can't get matched to a residency program. The AMA is actively lobbying to fix that problem.
"2 - We hear about long wait times in other countries. And the stories are mostly true. There's nothing wrong with waiting, but we've been conditioned to expect near-immediate resolutions."
Are you sure? I have to schedule several days if not a week in advance just to go to my PCP, much less a specialist. I also live in an area with no shortage of medical services.
Just making sure. Waiting a few days to see a GP isn't that weird.
If it's emergent (like a severe allergic reaction), there's the ER.
If it isn't emergent but needs resolving sooner (like an ear infection), there are Urgent Care clinics everywhere. I've also had the experience that my GPs' assistants can find time in their schedules if my problem is one that (1) they can resolve and (2) does need a quicker resolution.
Yep, I laughed the other day when I saw an article in WSJ that was talking about a billion dollar business responsible for putting drug ads in doctors offices. That billion dollars is coming from somewhere and I think I have a good idea of where.
It's complicated. The US spends more per capita (PPP) than any other country by good margin [1]. Of that, the US government pays roughly 50% of the total cost [2]. The net effect is that the US government already pays as much per capita as many European countries with socialized medicine.
In short, we have a cost problem that's not being tackled. Pharmaceuticals are often targeted, but they're about 8% of our total healthcare costs. We really need politicians that will tackle the other aspects of cost.
The countries that finance public healthcare have tax systems that are considered regressive by US standards. Some states have sales taxes, but we have no national VAT. As I understand it, some countries like Sweden have income taxes on lower income workers, whereas in the US, roughly 45% of households pay no federal income tax.
You can only squeeze so much money out of the wealthy, but the numbers don't add up to cover the projected costs of nationalized healthcare in the US. Taxes would need to be raised across the board. It's easy for campaigning politicians to propose pie-in-the-sky plans, but proposing a financially plausible one would be political suicide.
They are are already paying twice as much as any other developed nation with a "free-market" approach to healthcare. I do not understand the mental gymnastics to reach the conclusion that citizens as a whole would pay more in a single-payer system.
They might pay more taxes indeed, but their private insurance costs would disappear overnight.
As for healthcare costs inflation, that would quickly disappear with the transparency mandated by a single-payer system. One of the arguments explaining the always-rising healthcare costs in the US is a complete darkness from the consumer side on the actual price of the healthcare they are getting, thus allowing gouging at every level.
>I do not understand the mental gymnastics to reach the conclusion that citizens as a whole would pay more in a single-payer system
The reasoning goes like this:
The entrenched well funded (and money loosely translates to political power) interests influence the legislators doing the implementing in order to ensure a regulatory capture that allows them to continue swindling people at their current level but because it is now proxied through the additional overhead of government the net cost to the citizenry is greater than the current "get swindled directly" system and we have little/no net change in outcomes.
Basically people don't trust the government to not screw it up so badly that it actually costs more. I'm sure the cost would come down over time but with the high cost and uncertainty involved that's a tough sell.
Socialized healthcare doesn't mean doctors are a government employees. It's still private profit driven companies running their businesses. It's just the government instead of your insurance company paying.
A good deal of that cost is due to private insurance. The free market approach has resulted in middlemen inserting themselves into the healthcare pipeline and leech dollars from consumers.
It isn't the only reason, but it is one of the biggest.
US spent $3.65T on healthcare in 2018. or 3650 Billion.
Insurance Net Income was 23 billion. Or 0.63% of total US healthcare expenditures was 'profit' for insurance.
"But, public option will save the costs/salaries/buildings/etc that you pay to insurance." Yes, but not all costs. You'll need to make up a small difference.
But, let's assume we only count money paid to 'care'.
If we ignore all other costs associated with insurance and just pass the 'care' portion through. Insurance REVENUE was 706 bil - 600 bil (What was paid for care). or 106 bil.
So a maximum savings of 2.9%. So rather than spending $11,172 per person we're down to $10,836 per person for healthcare. A savings of $336. Still far and ahead above what other countries spend.
So realistically we'd see a savings of 0.6% to 3% savings.
> US spent $3.65T on healthcare in 2018. or 3650 Billion.
> Insurance Net Income was 23 billion. Or 0.63% of total US healthcare expenditures was 'profit' for insurance.
Profit is not the main source of the expense imposed by private health insurance, administrative costs are; Administrative costs are estimated at around $1.1 trillion nearly a third of the total, much of which, particularly billing and insurance-related (BIR) costs which account for about half of admin costs, would be eliminated in a single-payer or even public option systems, since the BIR costs imposed in current US public programs are far lower than private insurance (and some of those are still due to interaction with private insurance—e.g., coordination of benefits—and so would be erased even for public programs in a single-payer system.)
>since the BIR costs imposed in current US public programs are far lower than private insurance
Which is why I included this piece.
>If we ignore all other costs associated with insurance and just pass the 'care' portion through. Insurance REVENUE was 706 bil - 600 bil (What was paid for care). or 106 bil.
>So a maximum savings of 2.9%. So rather than spending $11,172 per person we're down to $10,836 per person for healthcare. A savings of $336. Still far and ahead above what other countries spend.
Last year insurance spent $92 Bil on admin. Even if we 'save it by half' (comparing the 56 bil from your link) our best case savings of 106 bil drops to 60 bil. Or a reduction of 1.6% in healthcare spending or ~$160 per person.
And hospitals will still have admin as they still have to bill the government.
The administrative cost imposed by private insurance on administration is not the cost spent by private insurance on administration. The biggest share of it is the administrative cost imposed on providers for dealing with private insurance (there is also a cost, in terms of coordination of benefits, imposed on public insurers). Your analysis, unlike the source I cited, entirely ignores administrative costs imposed by the private insurance system on actors other than the private insurers themselves, which misses the bulk of the costs associated with the private insurance system we have.
> And hospitals will still have admin as they still have to bill the government.
Missed responding to this piece before, but, sure: but, from the source I cited upthread, BIR costs imposed in the US big public programs (Medicare/Medicaid) is 2-5% of total cost, in the US private insurance system, it's 17% of cost. With single-payer admin will be nonzero, but it also won't be nearly 1/3 of total health expenditures, nearly half of which is related to billing and insurance.
You are looking at the wrong number. US insurances are bloated institutions full of bureaucrats that do things that shouldn't be done. So it doesn't matter if they make some profit or lose money. They are still a big waste of money.
You won’t find the single silver bullet that will solve all problems of US health care. Pretty much all players are inefficient so you will have to reduce insurance costs and hospital costs and drug costs and a lot of other things. Also don’t forget that the insurance bureaucracy also causes a lot of cost at doctors who have to hire people who deal with billing.
A good deal is that doctors and healthcare providers in other countries don’t make well into the $300k+ range. There’s a lot of money to be made in the US versus other countries. Without the insurance companies, who would have the power negotiate pricing with the providers? Americans don’t find government intervention palatable unless the person is over 65.
Recently the head of the Oklahoma Surgical Center was on [econtalk](https://www.econtalk.org/keith-smith-on-free-market-health-c...). That center was founded in the late 90s, had all their prices on their website, no insurance works with them and get their prices are effectively lower our equal to what they were twenty years ago and lower than at a regular hospital. On top of that the doctors make more when they work for this center than anywhere else.
One thing I learned from the episode is that insurance companies get a reward for the delta between their negotiated price and the price a uninsured person would pay. This creates incentive for hospitals to raise their base price tag. Of course their is more to it. I cannot recommend the episode strong enough.
To me the bottom line is that right now we don't have free market health care and we don't have socialized health care we have the worst of both. Maybe what we have is best received as crony capitalism health care.
That is very interesting. I had always thought that price obfuscation was good for both healthcare providers and insurance companies, since any price obfuscation is an advantage for the seller while the buyer is left confused about how much they are paying for what.
> Without the insurance companies, who would have the power negotiate pricing with the providers?
Healthcare costs have skyrocketed because of the negotiators. PBMs are the middlemen who negotiate healthcare prices between insurance companies and providers. I can't speak for hospitals and procedures, but in the pharmaceutical industry, it actually has led to a system where insurers and PBMs both benefit from drug prices increasing as opposed to decreasing. They aren't driving costs down, they are directly contributing to driving costs up.
Negotiation does not cause costs to rise, it’s because of lack of price transparency that let’s insiders play games.
Make all the prices public, and watch all the excuses disappear. No insurance company will be able to answer the government or employer when they find out another insurance company was able to obtain the same medicine or healthcare for a lower price.
I posted a link in a parallel thread to a surgical center that has all their prices on their website. Insurance companies refuse to work with them, supposedly for the reasons you state. So you are correct.
Yup. The UK has a particularly vicious variant of this - the nationalised state-provided monotlithic system has its weaknesses, but everybody in the media only ever discusses American-style privatisation rather than all the various hybrid models. The mere existence of the American system is kind of a threat to our system which currently has zero healthcare bankruptcies.
(People also misleadingly claim that the UK system excludes private provision - it doesn't, it's just that only a small fraction of the population has it and the tax advantages are nonexistant. Optical and dental are also mostly private.)
The irony is that the US system is nowhere near the “free market”. Subsidies abound for the rich and the poor and old get free single-payer healthcare in the form of Medicare and Medicaid. Meanwhile veterans also have an entire single-payer system for themselves.
The relatively few who “pay their own way” face incredible costs as few of the health providers actually compete for customers in an open and free market and so they charge crazy prices and get away with it.
It's not ignored. I don't know much about the German system, but I'm an immigrant from the UK and I much prefer the US system to the NHS, and I hear similar horror stories about Canada. Which is not to say the US system is good, just better.
In the US, when I need a doctor, I get to see one right away. If the doctor recommends an MRI or ultrasound, I get it right away. No six month waits, no cancelled surgeries, no doctor strikes (!), no government deciding how to prioritize my medical needs, etc.
What it ultimately comes down to is that medical resources are scarce (and always will be while medical technology is improving and thus some care is expensive), and having the government allocate them can be inefficient (governments are generally inefficient due to lack of competition, as are systems where the customer is disconnected from the cost).
And yes, I care more about my own health care and that of my kids than I do about the health care of some stranger thousands of miles away. I have okay corporate health insurance and so the system works better for me than for some. (Some would argue that regulation rather than economic freedom are to blame for those people's worse experiences, but I'm not going to get into that other than to acknowledge it.)
You might disagree with some of my perspective, but the snooty attitude that Americans are oblivious morons is unwarranted.
There can (and typically should) be a difference in one's personal preference and what one would advocate as public policy. Of course I am more emotionally attached to my own health and my kids than I care about one hypothetical unknown stranger thousands of miles away, just as you are. But if I stop and think for a moment I can't rationally justify a system that works well for 1 human (me) and works poorly for 100 other humans.
As a relatively wealthy and well-educated American with great insurance (and easy access to other jobs with benefit packages should my employment situation change), yes, I benefit from the American system. But I wouldn't vote for representatives that advocated it. We're not yet approaching something that's a little bit worse for 99% of the country and a lot better for the remaining 1%, and I'm sure we will have many fun debates as to where we should balance the equation as we approach that point. I would have to be pretty selfish to vote for something that's objectively worse for most people in my country.
However, it would in fact take an oblivious moron to advocate something that's simultaneously worse on average and also worse for them individually, and yet that's what we have in American politics today.
I'm quite familiar with the US health system; it's fantastic, best in the world for the top few percent, as good as the rest of the world for another group, poor to non existent for the rest of the population. Your fantastic health care comes at the expense of your poorer neighbours having essentially no health care. That you're ok with that could be considered a snooty attitude as well.
My point is that these other systems work, maybe people working at the FAANG companies, in financial services etc. might see a slight decrease in their quality of care, but the systems would all still work and would be much less of a share of your GDP.
> I'm an immigrant from the UK and I much prefer the US system to the NHS
Interestingly, my wife -- who moved from the US to the UK a decade ago, and has had quite a bit of interaction with the healthcare system since she's been here -- feels exactly the opposite.
Here we finally got the MRIs that were recommended but family couldn't afford years ago. Sure, we had to wait for 3 months and the doctor's visit + MRI cost us a total of $35 (hadn't reached the $120 yearly out of pocket limit) but it was a known non-emergency.
The same thing happens for everything. If it hasn't happened in America, Americans argue as if it is a theoretical idea that has never before been tried on Earth.
I wonder if we really have to wait a full generation with the "new conditions" (such as national healthcare) already in place for the bickering to taper off. That is, the discussion about how much downtrodden-ness is OK as long as shareholders get increasing value.
I mean, at one point for the hospitals to continue to operate at ever more profits you basically have to stop curing people and make them come back. You can combat that with more choices, but nobody is breaking up the banks, so why would they break up the big hospitals?
The Netherlands has private healthcare and private insurance companies and has the second best healthcare system in Europe. The price per capita is on Northern/Western European average at 5300 USD per person. World-wide we are the 8th most expensive country per capita which seems fair given our high wages.
So even though we have the second best healthcare system and pay an average price for it, people still want to nationalise our system and revert the privatisation. Because "privatisation bad". It truly baffles me that people think it will be for the best. Perhaps the price will go down to the 4100 USD per capita that the nationalised UK system has has but I'm sure our quality would also drop to UK levels (16th place in Euro Health Consumer Index).
Do you happen to know what's different between the model in the Netherlands vs the US?
Is the insurance provided by employers? In the US, most plans are provided and heavily subsidized by the employer (because the tax code makes that palatable vs paying employees more).
Do you have co-pays or deductibles? If so, how large are they? In past decades in the US, good plans had fairly low costs to the consumer ($20 GP visit, $50 ER visit was common). These days, because costs have gone up, many plans have converted to high deductibles with dedicated savings plans ($5000/year per individual OOP, but the person is allowed to save into a tax-deferred account that's a lot like our 401k retirement system, just used for health care).
Employers pay the biggest source of income of our healthcare system through the zorgverzekeringswet. They pay around 6% on the income of their employees next to the income tax. Second biggest part are the private insurance companies that sell insurance for around €90 to €200 per month. The yearly deductible for all healthcare in the base package is €385 to €885, you can set this deductible yourself.
Dental and physiotherapy are separate from general healthcare and have their own insurances and payment structures. They are all privately owned facilities. I usually pay my physiotherapist around €40 for a 30 minute session so I don't need insurance for it. But if you have regular appointments it would make sense to get private insurance for it.
We don't have a lot of co-pay (eigen bijdrage). There are some parts in regard to post-natal care where a co-pay is required. Also on hearing aids, dentures, orthopaedic shoes, medicine and non-ambulance transportation to a health facility.
Surely there's more of a rationale than just "privatisation bad"? That's the strawman version of the argument. How often are people denied coverage or put into bad financial circumstances?
Well,anecdotally,I am friends with a family where one of the spouses grew up in Canada. Their advice when we were planning a trip to Canada was to make sure not to get seriously ill while we were there. Not the first time I have heard of this attitude from Canadians or people from UK.
I do not have anything good to say about our "system" (except that the doctors and nurses themselves are many times exceptional), but I also have seen enough of government run systems to know that that is not not an answer.
You are presenting this argument as if people do not get worried about getting sick when traveling to the US. I can assure you that most people are extremely worried about that because of the insane costs involved and the problem of dealing with insurance.
Getting sick while traveling is always a crap shoot.
There are many Canadians who have been convinced that our health care system is crap by the usual suspects. It isn't.
Yes, if you live in a major center in the US (like near John Hopkins or Stanford Medical) and have great insurance, you will get some of the best health care in the world. The cost is your less wealthy neighbours are dying and going bankrupt.
What you (and most Americans) fail to understand is the states are separate entities, more similar to the EU than the provinces of Canada.
If California wants to have socialized health care for all it's residents, literally nothing is stopping them. Many states already have 100% government medical insurance for the poor.
The reality is, government run systems are an absolute nightmare. Similar to government housing, you only use it if you can't afford the alternative.
>No matter how many people say "but a well regulated mandatory multi-payer type of system is working in Germany" or "nationalized medicine is working in Canada" it's all just ignored and the argument continues anew.
Practically nobody is saying that a single payer system or tightly regulated multi-payer system hasn't worked anywhere (we all know Canada exists) or can't work in the US.
Everyone is arguing about the specific implementation because those are the details that make or break it. Anything would work on paper. Even free market with some good regulations to promote competition would probably work. It's the specific details of actually implementing something that works (and the ability of the people who would be doing the implementing to get those details right and not be corrupted by existing interests) that everyone is arguing over.
Everyone with a brain realizes that when it comes to big systems involving lots of moving parts the fine tuning is what makes or breaks them. Look at all the various social services programs that were kneecapped over the years because someone came along and made a few small changes or some key feature was compromised out of existence. Everyone is bickering over every detail because every detail has the ability to cause massive amounts of hardship when applied at a societal level if said detail is done wrong.
Simply put, healthcare is a hard issue because the stakes are so high that nobody is apathetic about it making compromise and consensus hard to reach.
> Even free market with some good regulations to promote competition would probably work.
One of the really interesting things about US healthcare is how much is spent on bureaucracy.
Consider, the average surgeon does ~400 operations per year and they generally make less than 600k/year. That’s 1,500$ per operation for the surgeon. Even with support staff, infrastructure, and materials, the average surgery should be under 10k.
Now let’s take an insurance that’s paying say 80% of it’s premiums for medical care. That’s 1 / 0.8 = a flat 25% price increase directly on top of whatever they add to healthcare provider’s costs in terms of additional paperwork and negotiation.
Similarly, before it goes to insurance the cost is inflated at the healthcare provider level to cover administrative costs like unpaid bill collections etc.
From my POV its fair for the support services to cost a lot. The theatre or the nurses or the equipment or really anything we can account to facilities or administration might cost a lot and thats generally kind of ok.
A junior programmer costs $250/hr from booz allen or whatever and I think a lot of people here understand why that is. They might not be able to fizz buzz so well but we expect the system to fizz and buzz eventually and expensively.
You can't add up what a plumber spends on beer or pays an apprentice and try to say what he should charge for his business.
What sucks is that despite the rhetoric theres actually no market. Want a market? Let people actually choose and make costs transparent.
By should I am speaking in terms of competitive markets resulting in prices reflecting the cost of production + minor profits.
Cosmetic surgery prices are generally reflective of costs including advertising etc. It’s not cheap by any means, but you simply avoid overhead occurring in other parts of US healthcare. Dentistry is another example where prices are generally reflective of costs, at least compared to say hospitals.
> Nobody is saying that a single payer system or tightly regulated multi-payer system hasn't worked anywhere or can't work in the US. Everyone is arguing about the specific implementation because those are the details that make or break it.
They are certainly arguing that such systems won't be effective in ths US in this discussion:
> Many on the left despise mergers and consolidation, and anything that has a hint of monopoly power. Except when it comes to government, education, and healthcare! Doesn’t a single centralized monopoly providing everyone’s healthcare seem like a bad idea? Why is it so bad in business and so good for health?
> That is very bad reasoning. Most things don't get cheaper when they get nationalized. There is some evidence healthcare may be different in this regard, but the point is: costs are not invariant under nationalization.
> We can't provide everyone with all the healthcare that they should get. There are never going to be enough doctors, equipment or hospitals. Sickness is literally an endless source of suffering and we all die of something - there cannot be enough medical assistance to deal with everything even if we devote everything we have to the healthcare industry. Rationing access to healthcare by people's economic contribution to society is just as fair as any other sort of rationing you care to come up with.
> There aren’t sufficient amount of people willing to do the highly undesirable work of caring for sick, contagious, handicapped, possibly dangerous people without money as the end goal.
Healthcare isn't a hard issue because the details are hard to figure out. Healthcare is a hard issue because millions of Americans work for companies and industries that are dependent on the status quo. One of the primary reasons for skyrocketing healthcare costs is the explosion of administration staff/costs in healthcare systems. And the private insurance industry has given rise to some of the largest companies on the planet.
Its difficult because the system has evolved to a place where the parasites in the relationship have grown so large that they can't be removed without serious damage to the host. Not overhauling the system is unsustainable, but doing so will absolutely incur huge economic consequences for a large part of the population.
> Even free market with some good regulations to promote competition would probably work.
That's not a free market then. This is the hardest part of the entire discussion: everyone is attempting to not exercise political power because they have these grand notions that politics can be done for the benefit of all. I'm not saying M4A is impossible (in fact, I would prefer it if I still lived in the states), but the fact of the matter is that the donor class will feel the sting of this transition, so we go off and Chase fairy tales where both the donors and the people rationing insulin can both coexist.
Ultimately you end up with contradictory notions like a regulated free market.
There are plenty of regulated free markets. Examples would be everything which uses mains power, phone lines or radiates rf.
Or stuff you eat or medicine. Or occupational products. Or... actually I think more things are regulated than aren't.
I guess my point is that when regulations apply to everything around us, is that really the sticking point or is it the potential for regulatory capture and limited user choice?
I think we're talking about different definitions of a free market then. To me, a free market is a market which is self-regulating or free from external regulation. It would seem to me that you define a free market as having some, arbitrary amount of regulation. If the amount of regulation is "under," that arbitrary bar, then it would be free. I don't really think this definition works, as the bar for what's "free" is arbitrary and would vary person-to-person, nation-to-nation, so it becomes a meaningless term.
I do have a prior, which is that I don't think any "free" markets exist in western nations due to broad consumer laws, plus applicable domain specific laws but interested in your perspective.
There are severe limits on what any of us can buy and/or sell and how we talk about it. A good kick starter for discussion would be an example of a free market as you see it.
If you are doing things with widespread societal impact generally society will have some things to say about that and their (perhaps slow and ham-fisted) means of expressing opinions about that is law and regulation.
As a consequence of seeing all fields as essentially regulated, I have a pretty low bar for free markets which is mostly "multiple parties can meaningfully compete and politicians do not completely determine that. Also consumers have a genuine choice.". This excludes China but kind of includes the USA, in many fields. But health care is weird.
As an example of my point of view, I think we can have laws that regulate carbon, material waste or other externalities and might be "onerous" but still have "free markets".
Has there literally ever been a case where a merger actually improved things for customers to the extent suggested by the merging companies? I certainly can't think of one.
In the case of hospitals, a system occasionally takes over a bankrupt hospital. That isn't particularly worse for the people that continue to have proximity to the services available at the hospital.
Apple agreed to acquire NeXT and its technology in order to bring back Jobs, when Apple was on the cusp of bankruptcy, was absolutely certain to die, and had no negotiating power. It wasn't a merger.
Also modern Apple devices are based on the NeXT's operating system and have nothing other than cosmetic and emulative compatibility with MacOS. OSX/macOS is NeXTStep on top of Mach.
>Apple agreed to acquire NeXT and its technology in order to bring back Jobs
Not really to "bring back Jobs". Jobs was not considered any kind of wonder CEO or miracle worker at the time. They wanted a new OS, as their own traditional Mac OS successor attempt had failed.
They also looked and negotiated with Be (for BeOS), so it wasn't that they wanted Jobs particularly.
It would just be a nice "back to roots" publicity side benefit, but nobody considered Jobs especially their potential saviour at the time...
Even if you credit all of their software to NeXT, Jony Ive was at Apple pre-NeXT-acquisition and it’s hard to imagine their turnaround going as well as it did without his work on the iMac.
>His followers are crazed and or ignorant cultists with zero design taste or sensibility.
Is that he has been awarded dozens of prestigious design awards and accolades from famous industrial designers?
Because all these have also "zero design taste"?
How about you overblow some of his wrong choices and obsessions (especially around 2015-2018), and ignore more than a decade of wonderful products, widely successful, praised for their design (looks and function), and well received?
Here's an Ive fanboy:
I’m have to admit being a bit baffled by how nobody else seems to have done what Apple did with the Macbook Air – even several years after the first release, the other notebook vendors continue to push those ugly and clunky things. Yes, there are vendors that have tried to emulate it, but usually pretty badly. I don’t think I’m unusual in preferring my laptop to be thin and light. Btw, even when it comes to Apple, it’s really just the Air that I think is special. The other apple laptops may be good-looking, but they are still the same old clunky hardware, just in a pretty dress. I’m personally just hoping that I’m ahead of the curve in my strict requirement for “small and silent”. It’s not just laptops, btw – Intel sometimes gives me pre-release hardware, and the people inside Intel I work with have learnt that being whisper-quiet is one of my primary requirements for desktops too. I am sometimes surprised at what leaf-blowers some people seem to put up with under their desks.
Yes, Ive was absolute shit, which is why Steve Jobs (widely known as a cuddly man who never had a sharp word to say), said
"If I had a spiritual partner at Apple, it's Jony. Jony and I think up most of the products together and then pull others in and say, 'Hey, what do you think about this?' He gets the picture as well as the most infinitesimal details about each product. And he understands that Apple is a product company. He's not just a designer. That's why he works directly for me. He has more operational power than anyone else at Apple except me."
But sure. I prefer the clunky beige form that ruled the world before Apple started making big design waves in computers.
A lot of people think that tmobile and metro PCS merger really benefited the mobile carrier industry.
While there were more companies before the merger, verizon and at&t were dominating that a long tail of small companies was not true competition.
When tmobile merged, it started to add a true 3rd competitor to the scene and they were the first to do a lot of stuff with unlimited data. Many people attribute verizon and at&t following suit to their initial move.
Of course this is speculation as no one can prove casual linkage between these events, but it seems pretty plausible.
I think sprint and T-Mobile merging would help create a real competitor to ATT and Verizon too. It’s just the nature of mobile networks that bigger is better.
I disagree here, with the disclaimer that I don’t have an incredible knowledge of this industry so my details could be inaccurate. I’m just an armchair quarterback.
Sure, Sprint is a dead carrier waking, but T-Mobile is already a competitor to Verizon and AT&T.
T-Mobile doesn’t need Sprint to compete with the other two at this point. They have the spectrum. They also have a 5G network rollout out with the lowest frequencies, which means they’ll actually have a coverage advantage.
Back to Sprint, they essentially can’t afford to build out 5G. But for consumers, they’re the cheapest option by far, especially when you consider their MVNOs like Boost Mobile. They also have a tremendous mess of spectrum that isn’t a very good situation for device interoperability and availability, nor is it good for rolling out 5G at all.
In other words, Sprint needs T-Mobile, but T-Mobile doesn’t need Sprint.
If Sprint cut costs and declared that they are the cheap, forever on 4G network, that would benefit price-sensitive consumers. Sprint’s competitive advantage would be that it doesn’t have to spend a lot of money on bothering to upgrade anything, or the marketing budgets that Verizon and the rest spend (I’d love to know how much of our monthly bill ends up on TV), and that their 4G network is good enough if you mostly care about price.
In my view this is the alternative that the corporations won’t even suggest to the public because it’s not as profitable. The people who own Sprint maximize their investment returns by selling to T-Mobile.
Sprint going bankrupt or being sold in pieces or in whole may even benefit the consumer more than Sprint being absorbed by T-Mobile, but the big three are never going to admit that.
Finally, what’s happening here is that you are unintentionally parroting T-Mobile’s own PR and lobbying efforts. T-Mobile put out news stories and press releases describing this exact scenario and how it benefits the consumer. They claim that they will truly do 5G right if they own Sprint, but I think they just want Sprint’s customers to be tacked on to their own.
> T-Mobile is already a competitor to Verizon and AT&T.
How come T-Mobile is consistently cheaper than ATT and Verizon? How come Verizon is the most expensive?
If the networks were the same, why would people opt to pay Verizon more? As far as I know, for coverage, Verizon > ATT > T-Mobile. It’s mostly a function of more towers, and I presume T-Mobile has the fewest.
I'm not sure if economists have developed some sort of model that would show when a consolidation would be beneficial in the long term for consumers, but I'd sure like to see one. We tend to not like it when firms collude with each other to control prices or stave off competition, in fact, we make it illegal to do so. But we rarely give them much trouble when they want to merge, which really isn't any different from collusion, don't you think?
I think there's differences of attention that make it different. When there's only one brand name, it invites a competitor from another market in. When there's three, but they all have the same policy, that's a bit different.
Recent airline mergers in the US have clearly been a net negative for customers, probably for this exact reason. All of the airlines already flew to basically all the major airports, so mergers simply served to reduce competition and worsen prices and quality of service.
On the other hand, until the recent consolidation, US airlines were a terrible investment, so perhaps it’s not a viable business without huge economies of scale.
There’s even a joke of “how to go from billionaire to millionaire? Buy an airline”.
If marginal services or businesses essentially /need/ to merge to survive it could improve things certainly, but in that case the extent suggested is usually slim to none since the alternative is foregone insolvency for both.
There are studies that a fragmented hospital landscape wit too many small hospitals are increasing risks here in Germany. Whether mergers would make matters any better I don‘t know.
Though it's definitely the exception, I found it nice when Patreon and Subbable merged. Everyone being on one platform, and the payment structure being consistent, was a plus.
It would be nice if the FTC did their job of breaking up conglomerates and preventing monopolistic competition. But Washington is like a plutocracy and the FTC wouldn't be serving the interests of all that network of money and favors being passed around.
Hospitals, healthcare, should not be a business. If money is the end goal, cheap + efficient medicine will be thrown away, it might not even be profitable ! A curse for a businessman.
Competitive markets tend to optimize large profits away. If someone is charging lots for less effective treatment, the expectation in a market economy is that a competitor will step in.
The analysis you present is not uncommon, where the businessman somehow gets to choose how much money he makes in a vacuum, a situation that doesn't really exist.
Ironically, lots of US regulations prevent providers from entering markets, letting providers that already have regulatory approval charge more. Some regulations are literally written with this as the goal (CONs, Medicare reimbursement rules designed to prop up small hospitals with emergency rooms).
For competitive markets to work, consumers need to be able to rationally shop around. The medical system is not even close to built in such a way. You cannot shop around when you are riding an ambulance to a hospital, and those with potentially terminal diseases usually prioritize living. The existence of insurance, which no one suggests we should go without, adds another moral hazard that encourages the consumer to be less price elastic.
It would be just as massive an overhaul to turn this sector into a truly competitive market as it would be to nationalize it.
Research suggests that emergency room costs are 7% or less of total healthcare spending in the US (some studies claim it's as low as 2% of total yearly costs). In other words, there's a lot of room for shopping around.
But in the current system you can't. Nobody will tell you the cost of operation or treatment. It's not even malice: nobody knows what it'll cost. The system efficiently avoids competition.
My comment was not made in a vacuum. It was intended to address the concern raised by jbeam that emergency situation in healthcare completely preclude the use of market dynamics. My point is that emergencies are only a small part of healthcare, and by themselves are not enough to derail the idea of bringing markets back to healthcare.
I'd argue its not a competitive market in many cases. There are limits on your doctor choice depending on your insurer. You cannot shop around for a treatment, the hospital lines one up connected to their doctor's network and your insurance.
Hospitals are not a “business”. They are non profit companies that rake in revenue and billions in profit while undermining the cost of care to Americans.
There aren’t sufficient amount of people willing to do the highly undesirable work of caring for sick, contagious, handicapped, possibly dangerous people without money as the end goal.
Don't underestimate how many people find meaning in care work, whether it's financially very well compensated or not so much. Look at places where healthcare is less subject to market forces, like substantial parts of the EU. You might get positively surprised.
And good compensation for health professionals can happen in a non-profit context too.
Medical professionals will notice if healthcare moves somewhat away from the market. They will feel safer investing energy without expecting market based financial compensation.
Compare to an free or open source project. A project that pays some contributors, but not others is a rather unhealthy situation. Such a project would have more difficulties attracting and retaining developers.
Don't underestimate what people will do for other than financial compensation, given suitable conditions.
My point is someone working in healthcare is also working for money as the end goal, and a doctor/pharmacist/nurse getting paid is also a business transaction.
And none of that would change under single payer (or, as someone else suggested, a German-style model).
Absolutely no one anywhere is suggesting doctors and nurses should work for free. Single payer advocates are only suggesting that we cut out the byzantine mechanism of the US medical billing regime, and let the American people pay health care professionals directly, with taxes, instead.
I’m also not suggesting single payer is a problem. I’m simply claiming that healthcare is a business, regardless of who is paying what. People wanting money for labor to provide healthcare is business.
Doctors and nurses will still make plenty of money. Govt jobs are on a pay scale as would medical jobs be. With less administration there'd be more money to go around as well.
How? I don’t see the general populace lining up to work at nursing homes to perform those duties for minimum wage. There’s an extreme shortage of people willing to work at nursing homes because the pay is not commensurate with the quality of life at work.
The two best healthcare systems in Europe are in Switzerland and the Netherlands. They went from nationalised to privatised. Nationalised healthcare systems tend to rank lower on the quality index.
And while the Swiss system is expensive, can you really put a price on your health? I'd rather have a good system (Switzerland) than a cheap system (UK).
The Swiss system is reasonable because there are government set limits on deductibles and co-pay. Insurance providers are also prohibited from discriminating based on previously existing conditions.
The services are also much cheaper than the US in general, even though Switzerland has some of the highest costs of living in the world. A routine visit at your doctor will cost at most a couple hundred dollars. Your deductible may be ~1000-2000 dollars and co-pay 10% up to ~7000 dollars after which your insurance must cover everything.
Swiss insurance will only cover you outside of your home canton up to twice the cost of having the procedure done in that canton, and only in emergencies. For that reason Swiss people are warned about needing emergency procedures in the US and Japan because it can bankrupt them.
Hospitals are run and funded by each state in Australia. I think a decade ago the federal government started to run a hospital in Tasmania, but they pulled out of it because it was ridiculous. There are also numerous private hospitals. GPs and specialists are largely privately operated. Comparing Medicare to a single nationalised hospital system is not accurate — it's more like a national health insurance system with membership fees paid by the tax system.
Obviously having a single purchaser of so many services allows them a large degree of control, but it isn't even a single payer system, since many health services require extra funds (even a routine doctor's visit requires out of pocket costs for many people, like $30 — that isn't cheap) although that's a recent change. There's also private health insurance and extra fees you can pay for nice service (like a room of your own).
Many on the left despise mergers and consolidation, and anything that has a hint of monopoly power. Except when it comes to government, education, and healthcare! Doesn’t a single centralized monopoly providing everyone’s healthcare seem like a bad idea? Why is it so bad in business and so good for health?
> Doesn’t a single centralized monopoly providing everyone’s healthcare seem like a bad idea? Why is it so bad in business and so good for health?
Because health shouldn't be run like a business, just like the fire department shouldn't be run like a business. The only metrics that should matter are patient outcomes and cost.
I think the problem with never-ending healthcare costs is that it isn’t run enough like a business. Any normal business decreases costs to survive. It appears healthcare is at 20% of GDP and rising forever.
There are three options. I'll call them options E, S, and G.
Option E is to run healthcare entirely as a business. Payment up front, and refusal to treat anyone without payment.
Option S is to take option E, but avoid immediately attributable deaths. Treat somebody at the emergency room, even if they don't have a line of credit with them. Patch them up enough to walk out the door, but don't treat the underlying issues without additional payment.
Option G is to treat patients before they reach death's door, when it is cheaper to do so. To give the preventative care that keeps costs down, even if somebody isn't able to pay for it. To treat public health as a public good, rather than as a series of purchases.
Option E is evil, to let people die unnecessarily. Option S isn't openly evil, but is stupid. It is where the US is now, and inflates the costs tremendously. Option G is to actually be good.
Preventative care might not save money, but in a nationalized system which is funded by tax collection, having participants healthy so that they can live longer and pay more taxes sounds like a good idea.
I feel like it's not only a moral argument, instead it's a better alignment of those who pay and are served by the system. At present, the goals of insurers and providers are very different from patients, partly due to profit-seeking, partly due to the disconnect in who pays for it (49% of US population receives employer-covered healthcare).
Huh, thank you. I hadn't known that. I tend to go with the monetary argument first, since it helps to convince people who are primarily self-interested. I definitely think that there is a moral argument for option G, and will stick to those arguments overall in the future.
you've inappropriately reduced this into three bins, ignoring all nuance which is the actual hard part of the problem.
in option G, how much $ do we spend on terminally ill patients in order for them to have a few more days with their loved ones?
or how about smokers who will as a result of their actions will cost spades more than "good souls"? or type 2 diabetics on dialysis?
this false trilemma is largely useless and only presents one side of a moral choice and even then ignores the other prickly of it (read: the people paying for this glorious utopia and where the lines are drawn when it comes to saying no)
Either the system we have today works because we put enough money into it, and therefore would continue to work if we nationalized; or our system has unjust failures that we should seek to rectify.
We already pay for our healthcare in the US, we just do it predominantly via employer-contributed job benefits, and existing Medicare/Medicaid. The money for the bulk of healthcare is already there, but there are people falling through cracks all the time.
Is your position that bringing everyone's healthcare up to Medicare's baseline is too expensive? Where is the extra cost coming from?
> Either the system we have today works because we put enough money into it, and therefore would continue to work if we nationalized; or our system has unjust failures that we should seek to rectify.
That is very bad reasoning. Most things don't get cheaper when they get nationalized. There is some evidence healthcare may be different in this regard, but the point is: costs are not invariant under nationalization.
> Is your position that bringing everyone's healthcare up to Medicare's baseline is too expensive? Where is the extra cost coming from?
Cost of providing the existing service is not the only cost worth considering. The other issue is opportunity cost of innovation. Right now there are powerful incentives for people to innovate in the healthcare space, particularly in pharmaceuticals. But also in prosthetics and the procedural space. Nationalization is likely to crimp those incentives, and thereby lead to less innovation over time.
> in option G, how much $ do we spend on terminally ill patients in order for them to have a few more days with their loved ones?
Zero. They would be explicitly avoided care if they are known being unable to return to work nor parent somebody (higher-order parenting such as grandparents, uncles, aunts count too).
I would argue that dedicating a larger part of a nation's output to healthcare is not bad in itself. In fact the better futures I can imagine all have very significantly broader healthcare provision. And we'd be spending more on health because we can.
Efficiency matters, of course, and a higher fraction of GDP spent on healthcare isn't per se better, either.
One problem with private provision of anything is that a company only cares about the revenue it can actually capture itself. Nationalised provision, using tax as a revenue stream, can look at whether something is beneficial on the whole even if it isn't directly paid for.
sorry but how then should the fire department be run? both seem resource constrained at both the macro and micro level.
my understanding is that at a macro level firefighters routinely "trade" regions for sake of better defending bigger or more important regions. it will have to be the same for health care: not everyone can afford a legion of 24/7 ICU nurses and ER physicians on standby when the end comes, even if .gov is footing the bill.
IIRC dems got killed for "death panels" when ACA was getting played up. there will always be death panels - someone who decides whether or not an additional dollar is warranted for any particular individual - so what inputs should we use to make those decisions in your opinion?
Look back at how fire fighting was when it was fully private. The whole thing seemed kind of stupid to everyone.
Multiple companies would show up at a house on fire, check insurance plaques, and then head home if they hadn't paid them.
If no one had paid them they'd let things burn, which sounds fine conceptually, but it's much cheaper to put out a fire early, and it has that awkward tendency to spread.
Exactly. Currently they're for-profit death panels in the insurance industry. And their metric is profit, not minimising death and suffering.
The UK approach to this is a board called NICE, which measures effectiveness and tries to set a cost-benefit level. What this means is that the UK is behind on leading-edge cancer drugs which cost a fortune for a few extra months of life, but makes sure that everyone has insulin. The US system is the other way round: some people get the life extension, some people die from lack of insulin.
(A surprising amount of healthcare rationing in the UK is simple waiting)
I think there's a difference between fire brigades that are private businesses and government owned fire brigades that have territorial jurisdiction and which apply common sense to their funding to ensure the most efficient service possible.
For instance, given that fire brigades are commonly city-level in the US and that American cities often have highly irregularly and interlocking shapes, it is plainly more efficient to trade a certain amount of funding to have the other city look after your dog leg. But there is a mandate on them to look after all structural fires in a certain area. They can pay someone else to look after it on their behalf, but the mandate remains. Territory and funds are exchanged. In other places, where fire brigades are run nationally or regionally, perhaps even individual stations will trade — "we specialise in rural fires and you specialise in urban fires, so you should take this newly urbanised region off our hands" "okay, but we will also take your newly urbanised funding off your hands". But it might also occur at the national or regional level and thus be central planning rather than business like.
But a fire brigade that is a private business will look after fires that are cheaper for them to put out than to burn. Perhaps they will put out a fire in a non-member's building since every neighbor is an important member — and then they might sue them for all their worth. But if they have no customers in an area because the people who live there do not have the money, then they might let the fire burn. Or they might say "we are liable for a hundred thousand dollars compensation if we don't put out this fire, but it will cost us at least a million to put out". (The local fire brigade will probably have to let some fires burn because they don't have the resources to put them out — it may be vastly too dangerous to get involved, but of a nature that, after a day of burning, it will be much safer. Here, the difference is the consideration — the question is the relative safety of attacking it vs waiting it out, rather than the relative costs of attacking it vs waiting it out.)
A mediate position could exist, where private corporations are allowed to get involved in the firefighting business, but if that were permitted, it would be a situation where the mandate remains and the private firefighters would be paid by mandatory payments from the property owners of the relevant territory. Unlike most businesses, they aren't free to pick what they do. A private supermarket can decide if they want to stock Mildew Milk or not. But a private regulated/mandatory firebrigade would have to put out the fire at Mildew Milk even though they've had a long running feud.
> The only metrics that should matter are patient outcomes and cost.
But the reason fire departments aren't run like a business is because fires spiral out of control and affect neighbours. That is not really the problem when we are talking about patient outcomes. Obviously we should all get exactly what we want without having to worry about physical constraints. But when we go from what should happen to what will happen the whole physics-and-reality problem sets in.
We can't provide everyone with all the healthcare that they should get. There are never going to be enough doctors, equipment or hospitals. Sickness is literally an endless source of suffering and we all die of something - there cannot be enough medical assistance to deal with everything even if we devote everything we have to the healthcare industry. Rationing access to healthcare by people's economic contribution to society is just as fair as any other sort of rationing you care to come up with.
> Rationing access to healthcare by people's economic contribution to society is just as fair as any other sort of rationing you care to come up with.
What's the thought process for the "fairness" of income based rationing? This doesn't seem that rational from either utilitarian or deontological angles. From my perspective it's a very unfair strategy compared to providing equal care to all people.
There isn't an argument that income based rationing is fair. The argument is that there is no fair rationing process, but we have to pick one. Income at least encourages people to work for what they get.
How else do we ration healthcare? Best looking people first? Oldest first? Youngest first? They all have terrible edge cases that are as bad as richest first.
We can't give everybody what they need because that is physically impossible. I don't want to die, so if we are going by needs I need permanent life support :(. That isn't even slightly practical, so we can't do that either - someone has to do without.
We could directly build more hospitals, train more doctors, etc. It is hard to see what would really change - there would still be horrible stories about edge cases where the system failed and there would still be a great need for more people. We have to draw a line somewhere - why not here? If we can justify going beyond the economic equilibrium, at what point do we stop pouring money into the healthcare system? A serious question which in my view has no satisfactory answer.
You don't see the difference between a private entity that is beholden to no one and a public entity that can be changed through political/democratic means?
You don't see the difference between an entity designed for profit and an entity of the people, by the people, and for the people?
You might not agree its the most efficient solution, but its not a logical contradiction to be against private monopolies but for public entities.
> Doesn’t a single centralized monopoly providing everyone’s healthcare seem like a bad idea?
No. It doesn’t “seem” like a bad idea. Go look at actual countries that do it - it works fine and it’s vastly cheaper than the US’s failed “system”.
That said, you don’t have to go all the way and have a single healthcare provider: a single insurer will do just fine - it works for Germany!
Also: what the heck is a non-monopoly government even supposed to be? Of course a government is a monopoly (it is all of us), you want lots of competing governments running the same things? Now that does seem like a bad idea.
> Why is it so bad in business and so good for health?
Because a business is answerable to shareholders and a government is (theoretically) answerable to the electorate. This keeps the incentives between politicians and people aligned much more than between a monoploy business and people.
Id wish for consolidated billing. Every time I end up in the hospital (which is about twice a year), I seem to end up with bills from 5-6 different providers. 1 from the hospital itself, a separate one from ER services, another from the pharmacy, one each from the specialists I see, another for lab work and yet another from radiology/imaging.
This bifurcation of billing makes an easy trap into falling into dilliquency because youre inundated with so many bills for the same visit that, even if you can afford to pay, you're like, "didnt I already pay for this?"
Seriously, the hospital near me seems to be a racket for Bill collectors. It seems no one is employed by the hospital proper and that theyre effectively all subcontractors that submit their bills directly to the end client, despite never being notified of that.
I cannot imagine a process like this where I hire a contractor to build a house at X rate, and they agree, and then all of the subcontractors bill me directly outside of the initial agreement. Maybe not the best analogy...
The podcast Arm And A Leg recently had an episode [0] which explains this practice of receiving surprise bills from unknown providers. The short version is that hospitals use staffing companies who do their own billing (I think they mention that the pitch to the hospital is that their lives are made easier by not having to manage the extra billing). These staffing companies are frequently owned by private equity firms so they have an incentive to try to bill outside of the system to extract more profit.
The whole podcast is worth listening to, not just this one episode, especially if you are frequently involved in the medical system.
The reason the doctors are contractors who bill separately is so that they can all be “out of network” and get 100x the rate without giving you prior notice.
The X rate is at least the negotiated professional rate, not necessarily the total bill.
Too often hospital care involves out-of-network doctors, that will bill directly as they may not have contract with your insurance. Knowing who'll be on duty ahead of time is not always if at all possible.
I can't read the article. Does it get into whether the hospitals actually merged process in any useful way? I worked at Kaiser when they were attempting to get their hospitals to share medical records (through SOAP). It taught just how home spun every hospitals IT is. Frankly, I'm a little skeptical much progress could have been made as a result of a recent merger.
Consolidation of IT systems should make them easier to protect but in practice it seems like the net result is any IT problem ends up harming multiple hospitals instead of just one. When the same chain owns multiple hospitals in a single market, all of them having IT problems at the same time is dangerous as the others can't pick up the slack.
IT consolidation only happens when it is prioritized, and in many cases you end up with some hybrid system of bastardized mapping/integration tiers rather than a pristine single environment. Healthcare IT also has the challenge of ridiculous amounts of highly specialized and largely turnkey systems, interop with other hospital and research organizations and of course the ever-present regulatory requirements that must be maintained throughout.
Didn't read the article but the headline is absolutely not a surprise.
Unintended consequences of PPACA made the system significantly worse. They let multiple industries consolidate using PPACA as an excuse. Yet no one will talk about it for political reasons. This happened across the board not just among hospitals. I am surprised UNH didn’t start buying out biotech companies to make drugs exclusive to their plans.
Quality? The peeps who are already make big money running hospital corporations are mainly interested in making more money. Where I work patients are actually to as customers in some interoffice emails...
Nor do business mergers in general. The benefit of mergers is that bigger companies have bigger benefits for top executives. For example, higher status, bigger paycheck and better car for the CEO.
Payers (insurers) are increasingly acquiring provider organizations as a cost control measure. The industry is gradually converging on the Kaiser Permanente business model.
I recently realized that hospitals in the US are for profit. So probably, the mergers do increase returns for investors? Which was probably the goal of the merger anyway.
Reduce management overhead and align merged facilities with cookie cutter standards. Ironically a lot of merged systems keep their previous IT infrastructure, so it becomes a big interfacing job rather than standardization.
Right and this is true for all the other mega-mergers. It doesn't improve quality or lower costs or any of the other lies the companies promise the SEC. It does increase shareholder value and cut jobs.
The reason you want smaller entities in private healthcare is that is reduces the size and impact of bankruptcy risk. Same reason you want smaller banks.
If you want competition to work you have to have sufficient excess capacity in the system to allow entities to fail and fail fast.
Not so much a case of big enough to cope, but small enough not to matter that much in the grand scheme of things.
That ought to be the rule of thumb for any competition authority - if this new entity went pop, would we notice?
Capitalism without the threat of bankruptcy is like Catholicism without the threat of hellfire. It no longer works as a concept.
In before, “This is proof positive free markets don’t work for healthcare”.
Excellent material for those interested, an actual cash only, price listed, customer facing hospital. Shiver ye comrades for the devil capitalist is and has been here.
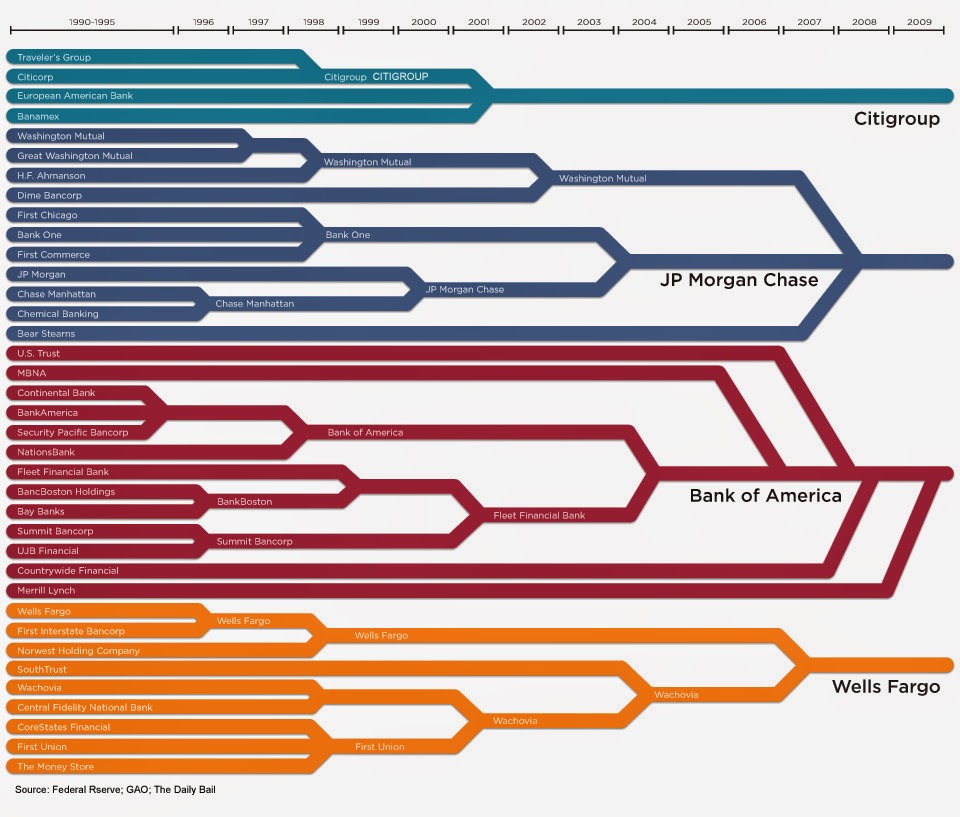{kind=link}
No matter how many people say "but a well regulated mandatory multi-payer type of system is working in Germany" or "nationalized medicine is working in Canada" it's all just ignored and the argument continues anew.